
Tennis players have an increased risk of injuries such as chronic overuse syndromes and acute traumatic injuries due to high demands placed on the body during training and competition. Data collected among tennis player playing in Wimbledon tournament showed that the shoulder joint were the most frequent site of upper limb injury, with internal impingement and SLAP tear being common overuse injuries.
What is a SLAP lesion?
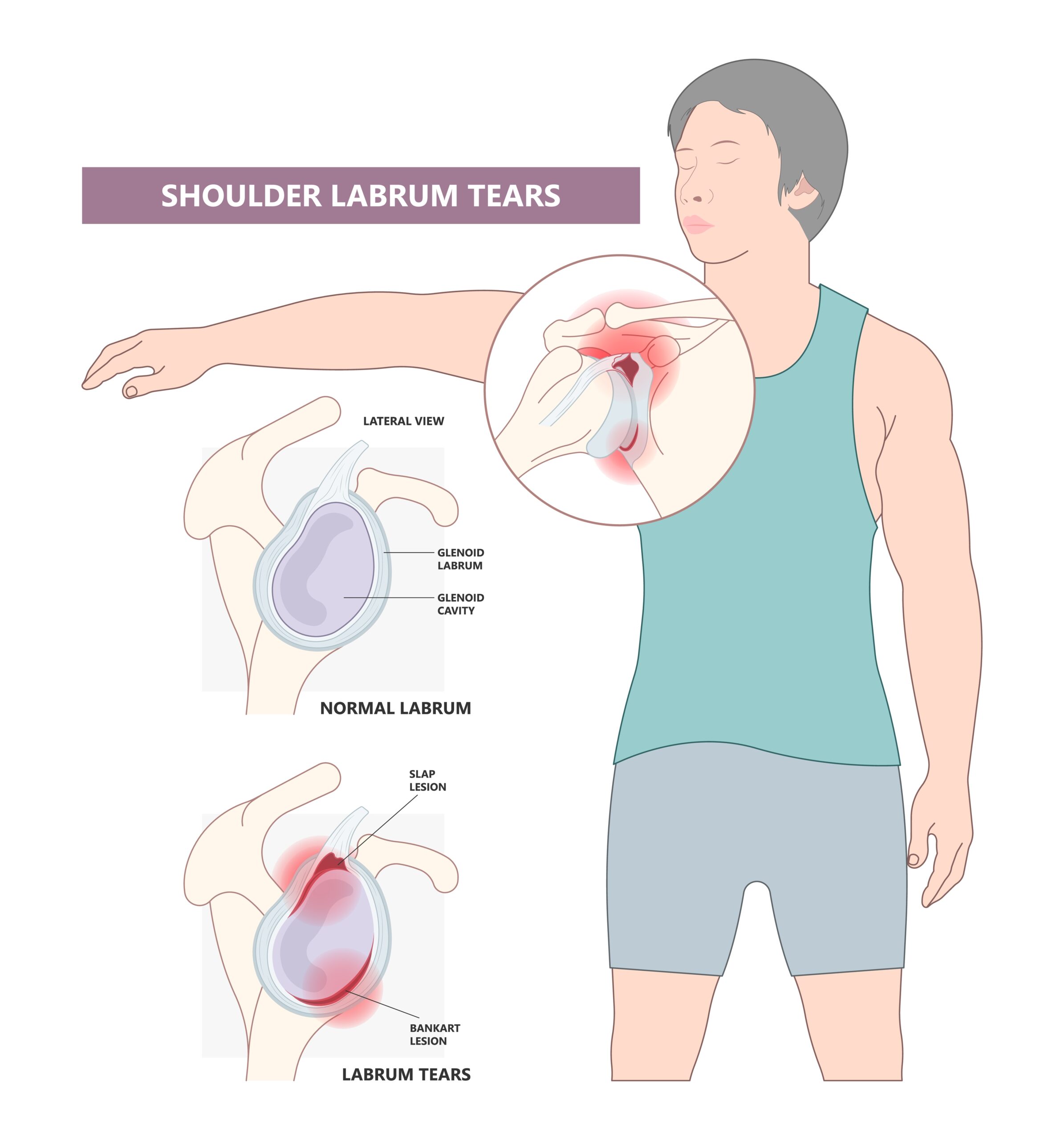
Superior Labral Anterior Posterior (SLAP) tears are injuries of the glenoid labrum. These injuries involve the superior glenoid labrum, where the long head of biceps tendon inserts. They may extend into the tendon, the glenohumeral ligaments or other quadrants of the labrum.
Mechanism of Injuries
These injuries can also occur due to repetitive throwing, causing repetitive microtrauma to the glenoid labrum when the shoulder is in abduction and maximal external rotation. This combination of movement creates a torsional force, resulting in “peel back” effect at the origin of biceps tendon and degenerative fraying of the labrum. Another cause of the injury is due to repetitive deceleration and follow-through component of a throwing movement.


Classification
SLAP tears can be classified into 4 types
Type I : Degenerative fraying on the inner margin of the superior aspects of the labrum
Type II : Long head of biceps attachment and the adjacent superior aspect of the labrum have pulled of the superior glenoid tubercle
Type III: Superior labral-bucket handle tear
Type IV: Superior labral bucket-handle tear extending into biceps tendon
Clinical Presentation
- Intermittent pain associated with overhead movements
- Painful clicking/popping with shoulder movement
- Reduced muscle strength and endurance of rotator cuff and scapular stabilizer muscle
Limited range of motion of shoulder internal rotation

How is it diagnosed?
Imaging method such as MRI and arthroscopy are considered the best tools to diagnose SLAP lesion. A combination of two sensitive tests and one specific test is used to diagnose a SLAP tear.
- Sensitive test: O’Briens test and apprehension test
- Specific test: Speed’s test, Yergason’s test, and biceps load II test
Management
- Grade I management: conservative, usually anti-inflammatory medications, cryotherapy, rest, and physical therapy
- Grade II, III and IV: surgery and post-op physical therapy
Physical therapy management
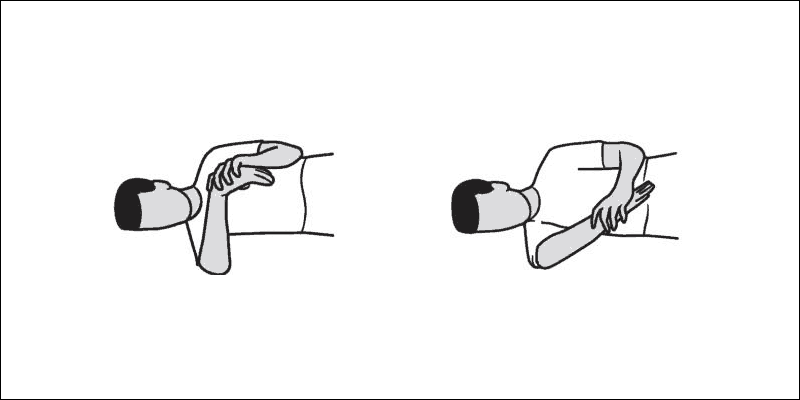
- Range of motion exercises of shoulder joint and sleeper stretch
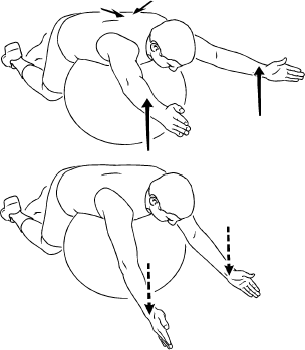
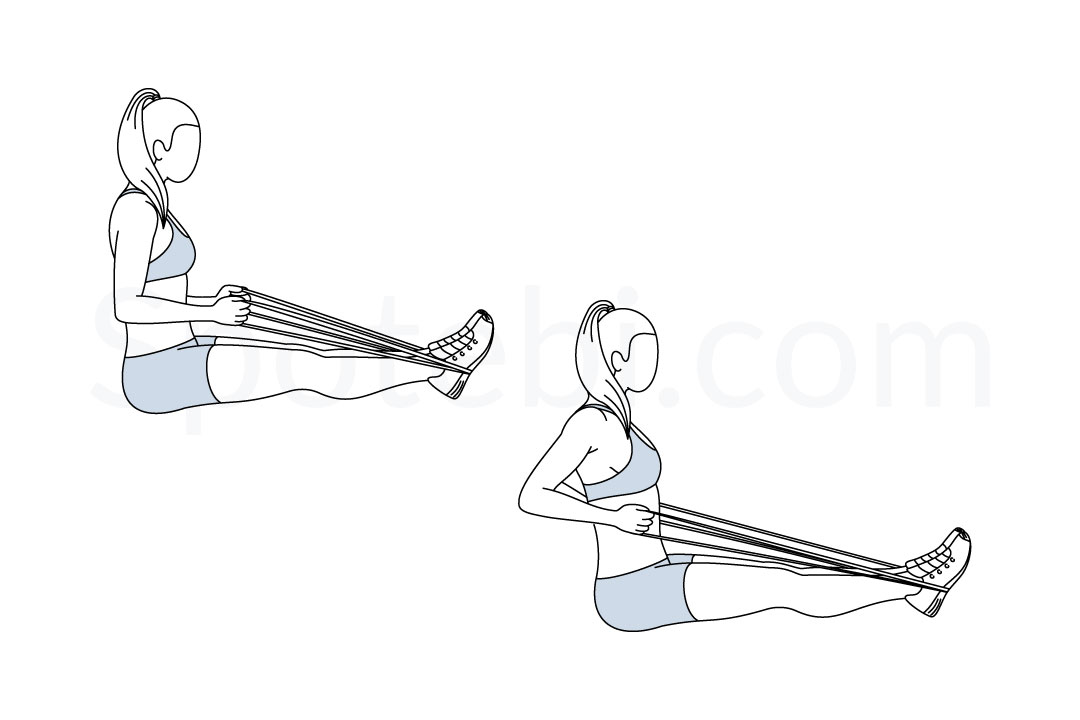
- Strengthening exercise for rotator cuff and scapular stabilizer muscle
- Pain management with cryotherapy, hot pack and ultrasound therapy
Exercises
- Sleeper Stretch

- External & Internal Rotator Strengthening

- Deltoid Lateral Raise

- Scapular Depression exercise

- Serratus Punch
- Rowing exercise



References
Majewska, J., Kołodziej-Lackorzyńska, G., Cyran-Grzebyk, B., Szymczyk, D., Kołodziej, K., & Wądołkowski, P. (2022). Effects of Core Stability Training on Functional Movement Patterns in Tennis Players. International Journal of Environmental Research and Public Health, 19(23). https://doi.org/10.3390/ijerph192316033
Sherry, M. (2011). Rehabilitation Guidelines For SLAP Lesion Repair. UW Health Sports Medicine Center, 1–6. http://www.uwhealth.org/files/uwhealth/docs/pdf/SM14888_SLAP_Repair6.pdf
Klatt, J. (2010). Grade I Slap Lesion : A Conservative Treatment Approach.
Slap Lesion. Physiopedia. (n.d.). https://www.physio-pedia.com/SLAP_Lesion
Prepared by:
Mohd Ridhwan bin Md Nadzri
Your Physio Cheras