
Ankle Sprain?
One or more of the ligaments that support the ankle stretch beyond their limits and tear.
Inversion-type, lateral ligament injuries represent approximately 85% of all ankle sprains. The incidence of ankle sprain is the highest in sports populations.
Ankle Sprains consist of:
- High Ankle Sprain:
- syndesmosis injury
- 1-10% of all ankle sprains
- Low Ankle Sprain:
- ATFL and CFL injury
- >90% of all ankle sprains

![]()
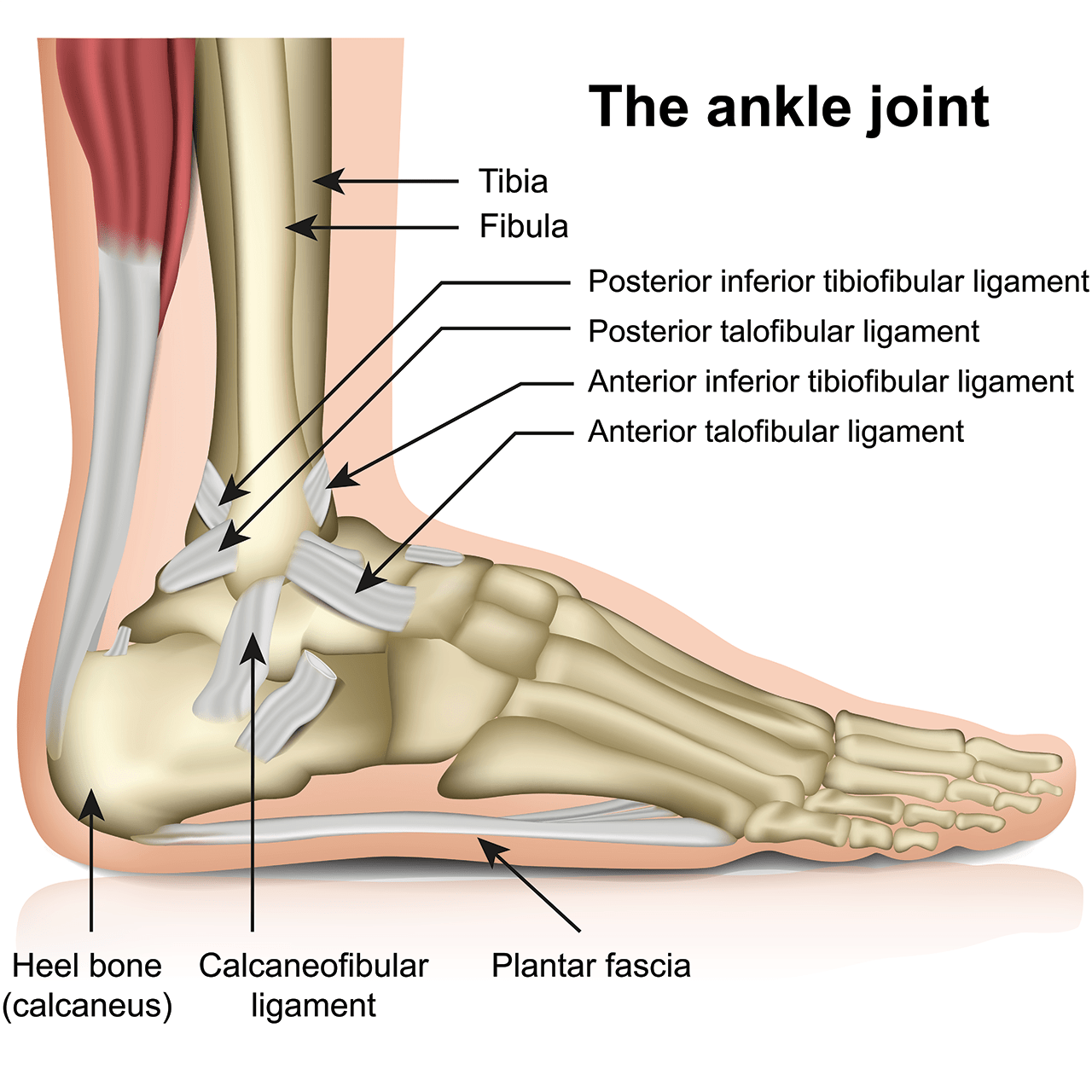
Anatomy of Ankle Ligaments
- Medial collateral ligament
- Deltoid ligament (ATTL, PTTL,TCL,TNL)
- Lateral collateral ligament
- Anterior talofibular ligament (ATFL)
- Posterior talofibular ligament (PTFL)
- Calcaneofibular ligament (CFL)
- Syndesmosis ligament complex
- Anterior inferior tibiofibular ligament (AITFL)
- Posterior inferior tibiofibular ligament (PITFL)
- Interosseous ligament(IOL)
- Transverse tibiofibular ligament (TTFL)
Risk Factors
- Sports Participation
- Uneven Surfaces
- Prior Ankle Injury
- Poor Physical Condition
- Improper Shoes

Clinical Presentation
- Pain with weight bearing (may or may not be able to bear weight)
- Tenderness when you touch the ankle
- Swelling
- Bruising
- Restricted range of motion
- Instability in the ankle
- Catching or popping sensation may occur following recurrent sprains

Physiotherapist use Special Tests to double confirm:
- Anterior drawer test: To assess ATFL (Castaing & Delplace, 1972)
- Posterior drawer test: To assess PTFL
- Talar tilt test: To assess CFL, ATFL and deltoid ligament
- Squeeze test: To assess syndesmosis rupture
- Kleiger’s test: To assess syndesmosis and deltoid ligament
Intervention
Pain Management
- TENS on ankle joint for 15 minutes.
- Therapeutic modalities like Shortwave diathermy, ultrasound or electrical stimulation are applied as adjunct treatment to mobility and stretching exercises to help reduce pain and increase ROM (Martin et al. 2013).
- Ultrasound on scar for scar tissues break down.
- Ultrasound used in this method can actually prevent some scar tissue from forming, and may be able to break some scar tissue down. (Belanger, A., 2003)
Myofascial Release
- Peroneal longus and brevis in supine lying to reduce muscle spasm.
- Myofascial release is a rehabilitation method frequently applied to restore optimal soft tissue length, decrease pain, and increase function (Greenman P., 1996).
Ice / Cold Pack
- Reducing metabolic demand
- Inducing vasoconstriction
- Limiting bleeding
- Reduce pain by increasing threshold levels in the free nerve endings and at synapses and by increasing nerve conduction latency to promote analgesia.
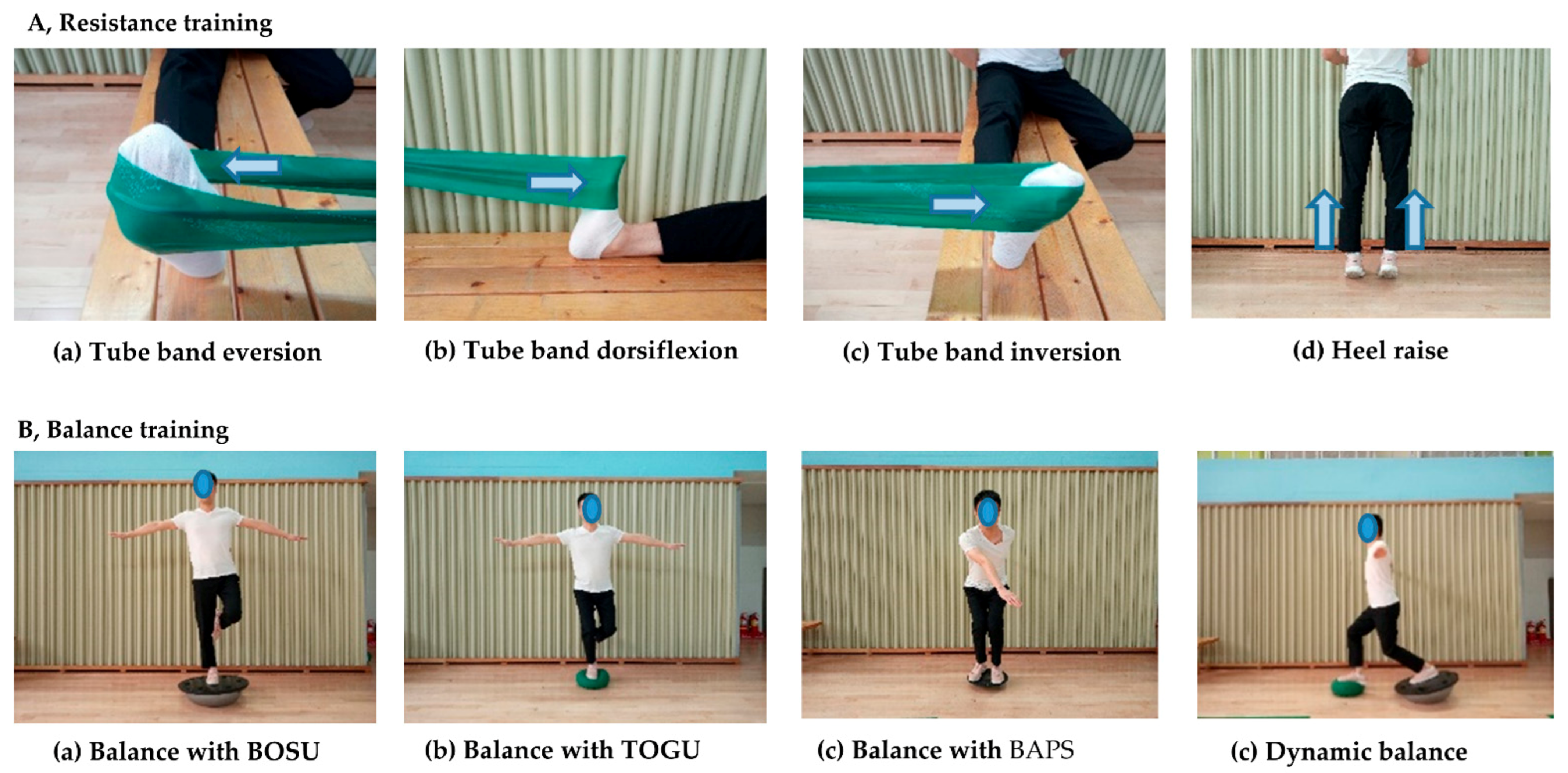
Therapeutic Exercises
Ankle Flexibility and Range of Motion Exercises

Resistance Training and Balace Training
References
Dijk, C.N.V., Mol, B.W.J., Lim, L.S.L., Marti, R.K. & Bossuyt, P.M.M. (1996). Diagnosis of ligament rupture of the ankle joint: Physical examination, arthrography, stress radiography and sonography compared in 160 patients after inversion trauma. Acta Orthopaedica Scandinavica. 67(6). 566-570
Hertel J, Denegar CR, Monroe MM, et al. (1999). Talocrural and subtalar joint instability after lateral ankle sprain. Med Sci Sports Exerc.31(11):1501-1508.
de Cesar PC, Avila EM, de Abreu MR. Comparison of magnetic resonance imaging to physical examination for syndesmotic injury after lateral ankle sprain. Foot Ankle Int. 2011;32(12):1110-1114.
Johannsen, A. (1978) Radiological Diagnosis of Lateral Ligament Lesion of the Ankle: A Comparison between Talar Tilt and Anterior Drawer Sign. Acta Orthopaedica Scandinavica, 49(3), 295-301, DOI: 10.3109/17453677809005768
Sugimoto, K., Isomoto, S., Samoto, N., Okahashi, K., Araki, M. (2017). Recent Developments in the Treatment of Ankle and Subtalar Instability. The Open Orthopaedics Journal, 11(4), 687-696
Prepared by:
Giselle
Your Physio Cheras